




Neuroprotective Strategies in Traumatic Brain Injury
Peter JD Andrews
Western General Hospital NHS Trust and University of Edinburgh, UK
Any severe trauma to the brain results in the activation of a cascade of biochemical pathways and release of chemical mediators. The innate response includes pro-inflammatory cytokines, chemokines etc., that are responsible for aggravating brain injury, that causes secondary injury long after the primary injury has occurred.1 The brain can be said to hold the ‘seeds of its own destruction’ and its response has been called the “secondary injury”. Secondary insults are measurable physiological derangements that include hypoxia, hypotension and fever, which exacerbate the neurological damage. Cerebral hypoxia leads to synthesis of prostaglandins, excessive release of cytokines, superoxides and complement activation, changes in vascular tone and oedema due to early cerebral barrier opening, loss of neurones, vessel damage, contusions and blood–brain haematoma expansion.2 Despite these observations, effective neuroprotective interventions are lacking. The very complexity of the biochemical response to injury in the brain is an obstacle to the development of neuroprotective medications or other interventions for use after a trauma has occurred. Although some interventions looked promising during in vitro and in vivo studies, they have not shown efficacy in clinical trials and thus neuroprotection following brain trauma remains a substantially unmet medical need.3
Preclinical models of neuroprotection have had numerous shortcomings. Ideally, these should evaluate the efficacy of interventions across different injury severities, they should be randomised and they should demonstrate efficacy with different classes of drugs in a clinically relevant time window. In addition, these studies should examine late functional and histological outcomes; they should determine the pharmacokinetics and brain tissue concentrations of drugs and evaluate their efficacy in a range of patient ages of different genders. The effects should be consistent in different animal species and in different laboratories.4,5
Some treatment modalities do provide neuroprotective benefit in brain injury.4,6,7 For example, following ischaemic stroke current treatments include recombinant tissue plasminogen activator and thrombectomy.8–11 Removal of intracranial haematomas and decompressive craniectomy have improved survival and possibly reduced subsequent disability. However, reducing intracranial pressure (ICP) alone has had little effect on favourable outcomes. One study that analysed a case series involving >125,000 patients, however, showed that from 1970 to 2010, the use of more aggressive monitoring and treatment in severe traumatic brain injury (TBI) had reduced mortality by 12% (p<0.001) and favourable outcomes were improved by 6% (p=0.0105).12
One particularly damaging aspect of TBI is fever. Core temperature can underestimate brain temperature by 1–2°C in TBI and elevated core temperatures have been associated with adverse outcomes in numerous studies.13–15 Several studies have shown that patients with TBI and other neurological lesions can spend extended periods with temperatures >37°C; in some (c. 20%) it can exceed 39°C and managing fever is critical 16 Fever is a potential modifiable risk factor and has also been associated with increased ICP.17 There have been no clinical studies comparing the effects of interventions such as fever prevention and induced normothermia in TBI, and trials are urgently needed. In stroke, however, several animal model studies, using the bilateral common carotid artery occlusion model, have shown differing results with no overall indication that such temperature control interventions have positive benefits.18–20 A meta-analysis of 23 studies showed that in terms of mortality, normothermia performs better than allowing fever to persist in patients with stroke, TBI or cardiac arrest. However, Cochrane Reviews have concluded that there are no completed randomised trials of modest cooling (36–37.5°C) for people with TBI, so this treatment cannot be currently recommended but trials of this intervention are needed.21 These reviews state that approximately 33% of patients currently receive some form of physical cooling after brain injury and >90% receive paracetamol but despite this, episodes of hyperthermia remain frequent. Paracetamol alone is ineffective at reducing neurogenic fever.
Most of the current understanding of brain injury-associated pathophysiology comes from rodent models of moderate injury. Many such studies continue to be conducted but they all face a fundamental problem of whether they are mimicking the human neuropathologies. If drugs are developed on the basis of tissue culture and these inadequate and potentially misleading animal models, they may well not be effective in the clinical setting.
An encouraging development in neuroprotection research is the use of nitric oxide synthase (NOS) inhibitors in brain injury. The phase IIa Nitric Oxide Synthase Inhibition in TRAumatic brain injury (NOSTRA) trial (n=32) has compared the efficacy of the NOS inhibitor VAS203 versus placebo in TBI.22 Six month results showed that VAS203 treatment produced no significant difference on ICP or central perfusion pressure (CPP) versus placebo yet treatment intensity and extended Glasgow Outcome Score were significantly improved (p<0.04 and p<0.01, respectively), but acutekidney injury was associated with this treatment.
Despite disappointments with recent treatments, there are many new therapeutic possibilities in neuroprotection after non-anoxic brain injury to be investigated. While outcome benefits of specific agents have not been demonstrated, major advances have been made by applying a package of clinical measures such as meticulous monitoring and careful prevention or limitation of secondary insults in the early phases after injury.
Targeted Temperature Management for Intracranial Pressure Control
Mauro Oddo
Department of Intensive Care Medicine and Neuroscience Critical Care Research Group CHUV-University of Lausanne, Switzerland
In patients with brain injury of differing types, fever and raised ICP are associated with worse long-term outcomes.23 Fever occurs frequently following brain surgery and greater numbers of febrile episodes are associated with increased length of hospital stay.24 Targeted temperature management (TTM) is frequently employed to manage fever after TBI. Clinical physiological studies show that TTM after TBI has positive effects that include reducing ICP, brain temperature, brain glutamate, cerebral metabolic rate of oxygen (CMRO2) and cerebral metabolic distress. The negative but controllable effects of TTM include increased shivering that affects systemic and cerebral oxygenation, and may require increased sedation.25 The use of TTM may eliminate the need for antipyretic mediations, which eliminates their beneficial effects on reducing mean arterial pressure and CPP.
Despite the generally accepted importance of maintaining normothermia after TBI, the existing guidelines provide little instruction on how it should be achieved.26 In addition, there are few prospective trials that demonstrate the benefits of temperature management. The American Heart Association/American Society of Anaesthesiologists recommend that temperature management is part of basic support and a normal temperature is reasonable (Class IIa level of evidence: C).27 They also state that the effectiveness of therapeutic hypothermia before brain swelling is not known (Class IIb, level of evidence: C).
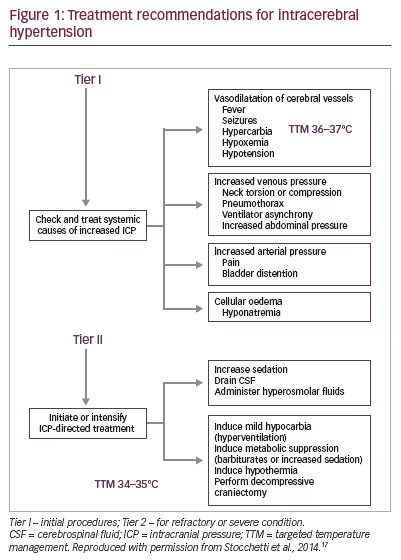
The European guidelines recommend that in patients with intracranial hypertension the causes should be initially treated by addressing factors such as fever, seizures, causes of arterial or venous pressure and cellular oedema (Tier I). If this fails, further measures should be taken (Tier II), which include: increased sedation, cerebrospinal fluid drainage, metabolic suppression and hypothermia (see Figure 1). Guidelines from France recommend three steps in which patients whose central temperature is >38°C should be cooled to a target of 37°C using various methods including paracetamol and external physical cooling (step 1). If that fails (>38°C for 4 hours) or during the acute phase (days 0–7 post-injury) or when patients have an acute cerebral lesion, treatments include: cold isotonic fluids delivered by intravenous catheter, surface cooling and thermal modulation to a target 37°C (step 2). If that fails, the treatment in step 2 should be intensified and solutions can be administered via a peripherally inserted central catheter to a target temperature of 35–37°C 28
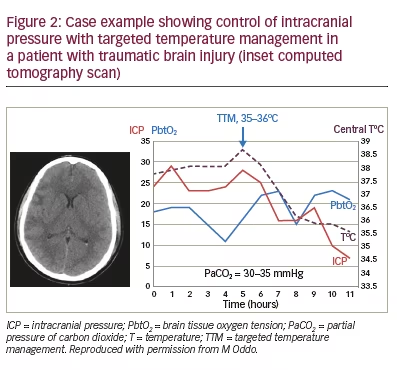
Clinical experience suggests that cooling tends to be beneficial after TBI.29 This is illustrated in a case example of a patient with TBI who was cooled using TTM, to 35–36°C, starting 5 hours after injury (see time profile in Figure 2). This reduced the central temperature from 38.5°C to 35.5°C over the following 6 hours and at the same time reduced ICP from 34.5 to 27.0 mmHg. During this cooling period, brain oxygenation was maintained and carbon dioxide levels were within 30–35 mmHg. In this patient, active cooling was stopped after 4 days and the ICP remained stable, sedation was stopped the following day and intracranial monitoring was removed.
Two further case examples in which TTM was a valuable treatment option are shown in the box below (see Figure 3 for associated computed tomography [CT] scans). These show that, in patients with severe TBI who have received other therapy, TTM reduces elevated temperature and ICP, and appears to improve outcomes.
A 27-year-old male had severe TBI, a Glasgow Coma Scale (GCS) score of 6, and a CT scan showing cerebral oedema and non-surgical contusions. His ICP was elevated >20–25 mmHg despite optimal sedation, moderate hyperventilation and a temperature of 37.8°C. He was given TTM and osmotherapy, which reduced the temperature and ICP, leading to a favourable outcome.
A 26-year-old male had severe TBI and GCS score of 5. On Day 1 post-TBI, a CT scan showed diffuse cerebral oedema. ICP was 20–25 mmHg with spikes >25 mmHg associated with brain hypoxia (PbtO2 <20 mmHg). He had been treated with deep sedation (propofol and sufentanyl), moderate hyperventilation (PaCO2: 31 mmHg), osmotherapy (hypertonic saline) and his temperature was 37.5°C. He received TTM therapy adjusted to control ICP<20 mmHg. This reduced ICP, leading to a favourable outcome.
- Fever and ICP are frequent and hazardous consequences of an insult to the brain such as TBI.
- Maintenance of normothermia is recommended but there is little consensus guidance on how to achieve it.
- The two case examples above show that surface cooling TTM can control elevated temperatures and elevated ICP in patients with TBI after other treatments have failed.
- Further case examples and case series also show a beneficial effect of surface cooling TTM in patients with TBI in controlling elevated temperature and ICP.
- An early analysis of the Eurothem3235 study showed no benefit from TTM in TBI, however, the control (standard care) patients were maintained strictly in normothermia and many were actively cooled, which may have confounded the results.
Targeted Temperature Management in Subarachnoid Haemorrhage
Emanuela Keller
Neurocritical Care Unit, University Hospital Zurich, Switzerland
Patients with subarachnoid haemorrhage (SAH) can benefit from hypothermia, but the mechanisms by which this occurs are poorly understood. The pathophysiology following SAH is complex. Cerebral blood flow (CBF) through the capillaries is affected by several factors including cerebral vasospasm (CVS) but also by CPP and resistance at the arteriolar and possibly venous levels. Alterations in the latter two factors may manifest as slowed circulation time and poor vessel filling as seen on angiography, but these cannot necessarily be correlated with CVS.31 Following SAH, there is a strong inflammatory response that is induced by the breakdown of erythrocytes in the subarachnoid space. This reaction induces secondary ischaemia due to vasospasm but also contributes to the development of brain oedema. To prevent such oedema, early intervention in the inflammatory cascade is essential.32
The damaging effect of inflammatory cytokines was demonstrated in a study of 138 patients with SAH.33 Unfavourable outcome (Glasgow Outcome Scale [GOS] 1–3) and delayed ischaemic neurological deficits (DINDs) were significantly associated with elevated blood Interleukin 6 (IL6) levels during the early phase (p=0.023 and p=0.026, respectively). It was suggested that IL6 levels could be a useful parameter to monitor following SAH. A pilot study (n=15) reported that IL6, tumour necrosis factor α (TNFα) and IL1β increase in blood and cerebrospinal fluid in patients after SAH, although IL6 was at 100-fold higher levels in CSF than blood.34 Hypothermia, with a target range of 33–34°C using combined therapy with endovascular cooling and barbiturate coma, markedly reduced both IL6 and IL1β (p<0.001 for both) indicating its efficacy in attenuating the inflammatory cascade. The ratio between IL6 levels in the CSF and plasma, as a parameter for intrathecal synthesis, furthermore, was significantly lower in patients who received combined therapy compared with those who did not receive it (p=0.014). Other work on adult rats indicates that hypothermia reduces vasospasm and decreases the reduction in CBF and oxygenation following SAH but the greatest benefit is gained when the treatment is within hours after aneurysm rupture.35
Cooling the brain in SAH is likely to reduce metabolism, however, the optimal target temperature has not been determined. Some studies have shown that, while patients are cooled, uncoupling between CBF and CMRO2 occurs to the extent that CBF exceeds the metabolic demand. This phenomenon is known as luxury perfusion.36 This concept was supported by a small case series of patients with SAH and hypothermia (33–34°C) provided some preliminary evidence of hypothermia-induced luxury perfusion in which a larger decrease in CMRO2 (54.3%) compared with CBF (35.7%) was observed.37
Fever is the most frequent symptom in SAH, occurring in approximately 75% of patients, and is strongly associated with death or severe disability as outcomes.38 In SAH, fever is more common than hyperglycaemia, hypertension, pneumonia and delirium. A meta-analysis of 24 studies in 2010 found that fever during acute hospitalisation for SAH was consistently linked with worsened outcome and increased mortality.39 Antipyretic medications, surface cooling and intravascular cooling may reduce fevers but the benefits from these measures may be offset by the negative consequences of shivering.39 The potential negative consequences of fever reduction were also indicated by a study of 21 consecutive aneurysmal SAH patients who were given diclofenac.40 This treatment effectively reduced body temperature but this led to 10% decrease in mean arterial pressure and CPP (p<0.001) and a 13% decrease in PbtO2 and brain hypoxia in 38% of patients. This suggested that fever reduction in SAH using diclofenac is not always beneficial and should be exercised with care.
Intravascular cooling can also be associated with thromboembolic events. In a study of 122 patients, among those with central venous lines (n=79) 5% had deep vein thromboses (DVT) or pulmonary embolism (PE).41 Among those with endovascular cooling catheters, however, (n=43) 37% had DVT or PE (52% in those treated for fever and 23% for those treated with hypothermia). In the treatment of fever in SAH, therefore, there is a need for prospective controlled trials that investigate the side effects; they should possibly use surrogate markers to determine outcomes, such as cerebral haemodynamics and metabolism, inflammatory response and secondary brain injuries.
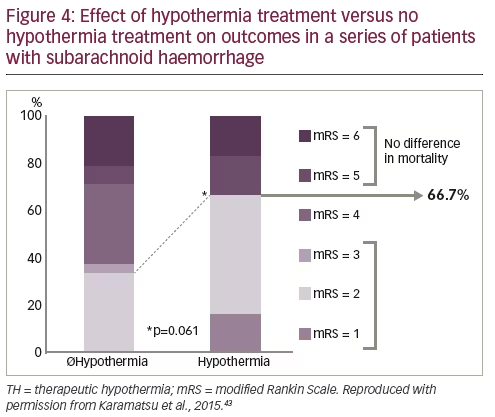
Hypothermia was applied in a study of 441 consecutive patients with SAH in which 100 patients developed raised ICP or symptomatic CVS that was refractory to treatment.42 Patients were treated with TTM using ice, water blankets or intravascular cooling (33–34oC), which was maintained until ICP normalised, CVS resolved, or there were severe side effects. Among these patients, with the most severe SAH, only 25% with raised ICP, 57.1% with CVS and 26.5% with ICP/CVS showed favourable outcomes (GOS 4 or 5). It was concluded that prolonged systemic hypothermia should be considered a last resort option in SAH with raised ICP or CVS that is resistant to treatment. In a more recent study, therapeutic hypothermia (TTM) was applied prophylactically early after SAH.43 A group of 12 patients with SAH who received early TTM (within 48 hours) showed reduced delayed cerebral ischaemia (DCI) and microvascular spasm compared with 24 matched patients from an SAH database. TTM significantly decreased macrovascular spasm and peak Doppler blood flow velocities (p<0.05). The frequency of DCI was reduced from 87.5% in non-TTM to 50% in TTM-treated patients, creating a preventive risk ratio of 0.33 (p=0.036). Favourable functional outcomes were significantly more frequent in TTM-treated patients (66.7% versus 33.3% of non-therapeutic hypothermia-treated patients, p=0.06; see Figure 4).
- Animal studies have improved the understanding of SAH pathophysiology.
- Intravascular catheters are associated with increased risk of thrombosis.
- Larger retrospective case series show that TTM is a last-resort treatment for intracranial hypertension and vasospasm.
- Findings of a recent prospective pilot study suggest that TTM treatment may be beneficial in high-grade SAH patients.
- A prospective randomised study in high-grade patients with prophylactic TTM is needed and should include a few centres with a very strictly controlled treatment protocol.
Targeted Temperature Management in Intracerebral Haemorrhage
Gregor Broessner
Department of Neurology, Medical University of Innsbruck, Austria
Intracerebral haemorrhage (ICH) has a very poor prognosis, with a case fatality of 40% at 1 month increasing to 54% at 1 year; only 20% of patients regain functional independence.44 Incidence of ICH varies from <37/100,000 in Europe to >100.9/100,000 in China and South-East Asia.44 In a study of 1,155 patients in a neurologic intensive care unit (ICU), mortality was 28% for spontaneous ICH, 27% for SAH and 27% for malignant/complicated ischaemic stroke.45 Outcome in ICH depends on various factors including ICH volume, re-bleeding, intraventricular haemorrhage, peri-haemorrhagic oedema development, comorbidities and withholding therapy. Among various critical interventions, it is important to consider the possible benefits arising from TTM in ICH management.
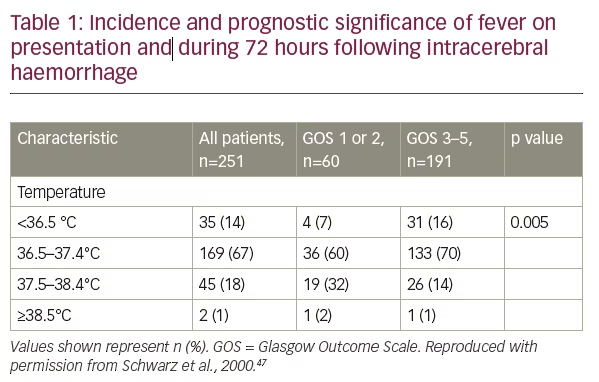
In patients with ICH, the incidence of fever is high.46,47 When patients have fever at presentation and during 72 hours after ICH there is a strong association with poorer outcomes as demonstrated in a study of 251 patients in which only 14% of those with temperatures of 37.5–38.4°C and only 1% with temperatures ≥38.5°C had GOS scores of 3–5 (see Table 1).47 This study also showed that the duration of fever ≥37.5°C for 24–48 h increased the risk of poor outcome (odds ratio [OR] 8.33) and was further increased for durations >48 hours (OR 13.52). Further evidence comes from a meta-analysis of 39 eligible clinical studies that included a total of 14,431 patients.48 This showed that fever was significantly associated with worse outcome, in patients with various acute severe neurologic diseases, as determined by multiple measures including mortality, GOS, Barthel index, modified Rankin Scale (mRS), Canadian Stroke scale and ICU length of stay.
Lesions in the central pathway of thermoregulation may cause central fever. This argument is supported by a study of 95 patients with ICH (30 with central fever) in which any thalamic involvement, larger ICH volume and intra-ventricular extension of the ICH were significantly associated with poorer outcomes (p=0.053, p<0.001, p<0.001, respectively).49 In total, 68% of patients with infectious fever, 86% of those with central fever and 34% of those with no fever had an mRS score of 6.
An important question is whether patients with ICH and early, noninfectious fever should be selected for TTM. Currently, the evidence supporting this intervention is uncertain; the European Stroke Organisation guidelines state that there is insufficient evidence from randomised controlled trials to make strong recommendations for early fever treatment after acute ICH.50 However, these guidelines also state that the treatment of fever after ICH may be reasonable (Class IIb, level of evidence C).
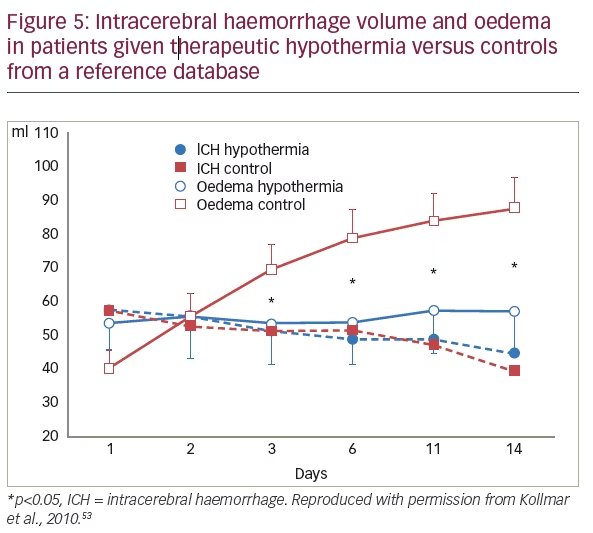
Numerous animal experiment studies of spontaneous ICH indicate a generally positive effect of TTM on aspects such as oedema, blood– brain barrier integrity, inflammation and thrombin-induced injury, but data from large studies on the benefits in humans are substantially lacking.51 Among smaller clinical studies that have been completed, one that included 41 patients with ICH showed that fever was significantly reduced in patients receiving prophylactic catheter-based versus conventional cooling (p<0.0001), but the study was underpowered to detect outcome differences.52 This intervention was not associated with increased major adverse events. A smaller trial of 12 patients with ICH needing mechanical ventilation showed that TTM of 35°C for 10 days stabilised oedema volume (as determined by CT scans) from 53 ± 43 ml at Day 1 to 57 ± 45 ml at Day 14, all patients survived and TTM resulted in no significant side effects.53 In 25 matched patients, managed without TTM and drawn from a haemorrhage data bank, oedema volume markedly increased from 40 ± 28 ml at Day 1 to 88 ± 47 ml at Day 14, and 7 patients died (see Figure 5). These preliminary results might indicate that TTM could prevent increases in peri-haemorrhagic oedema in patients with large spontaneous ICH.
Further supporting evidence came from a study of 25 consecutive patients with ICH.54 This showed that reduced peri-haemorrhagic oedema and favourable outcomes (GOS 3) were more frequent in patients who had received 8–10 days of 35°C TTM treatment than in 25 historical controls who received no TTM. Side effects were frequent but manageable with TTM. Another study (Systemic Normothermia in Intracerebral Hemorrhage, [SNICH, NCT02078037], n=100) that aims to determine whether prophylactic forced normothermia using surface cooling pads (Arctic Sun® 5000; Bard Medical, Covington, GA, US) in patients with ICH leads to less systemic inflammation and decreased peri-haematomal oedema is currently in progress with results expected soon.55 A further study, the phase II Safety and Feasibility Study of Targeted Temperature Management After ICH (TTM-ICH, NCT01607151, n=50), is investigating 72 h of TTM to 32–34oC and is also due to release findings soon.56
- Management of spontaneous ICH patients is complex with, as yet, no specific treatment.
- Fever is common and associated with poorer outcomes in ICH.
- Predisposing factors for fever are: haematoma location, ICH volume, intraventricular haemorrhage and infections.
- Strict normothermia/hypothermia might reduce oedema/ICH growth.
- Stringent avoidance of fever should be investigated in a randomised controlled trial, which should:
– compare hypothermia with controlled normothermia; and
– include patients with central fever.
Targeted Temperature Management for Seizures
Janneke Horn
Academic Medical Center, Meibergdreef, Amsterdam, The Netherlands
Refractory status epilepticus (RSE) is a serious condition with potentially harmful, even lethal, outcomes yet surprisingly many hospitals have no protocols for treating the condition. Current guidelines recommend the use of a benzodiazepine as first-tier treatment during the first 5–20 mins of the seizure. If that fails, however, there is no evidencebased therapy for second- or third-tier therapies for use 20–40 mins and 40–60 mins into the seizure 57 Options for second-tier treatment include: fosphenytoin, valproic acid, levetiracetam or intravenous phenobarbital. In cases where seizures continue, third-tier options include repeating second-tier medications or anaesthetics such as barbiturates, ketamine, thiopental, midazolam, pentobarbital or propofol (with electroencephalogram [EEG] monitoring), hypothermia or electroconvulsive therapy. In some patients, super RSE develops, in which status epilepticus (SE) continues or recurs despite 24 hours of continuous anaesthetic infusion.
A recent international patient registry of SE with a total of 488 cases from 44 countries found that 67.7% of patients received treatment within the first 6 hours of the seizures starting and the most widely used anaesthetic was midazolam followed by propofol and barbiturates.58 Control was achieved in 74%, a poor outcome occurred in 39.3% and good outcome in 36%. In total, 24.6% of patients died and 24.1% were severely disabled. The causes of SE recorded in the registry were various including: drug withdrawal, genetic factors, cerebral tumour, trauma, mitochondrial disease, vascular cause (e.g., stroke), acute meningitis and unknown factor. The registry also reported 347 cases in which ‘other’ therapies were used. These included: steroids (39.2%) intravenous immunoglobulin (20.0%), ketogenic diet (13.0%), hypothermia (8.4%), plasma exchange (7.2%) and neurosurgery (2.0%).
A small study (n=4) demonstrated the benefits of moderate TTM in SE.59 Patients were cooled to a target 31–35°C, which stopped seizure activity in all four patients allowing midazolam infusions to be discontinued and three achieved a burst-suppression pattern on EEG. After rewarming, two patients remained seizure-free but all showed reduced seizures. Adverse events included shivering, coagulopathy and thromboembolism. It was concluded that TTM could be used as an alternative or an adjunct to anaesthetics but larger trials are needed to evaluate its safety and efficacy.
The beneficial effects of TTM in SE are believed to result from its neuroprotective action that reduces brain damage and neuronal loss. TTM also reduces metabolism in brain tissues and conserves energy. This is supported by studies in rats in which normothermic animals in RSE were seized for 4.1 ± 1.1 hours and showed extensive damage in multiple brain areas and breakdown of the blood–brain barrier.60 Animals that were treated with deep hypothermia (20°C), however, showed termination of RSE within 12 minutes and showed reduced EEG power and seizure activity on rewarming and there was no SE-induced neuronal injury in most animals. The mode of action of such deep TTM is unknown but it may alter ion pump function, change membrane properties and alter voltage-gated ion channels. It may also slow release of excitatory neurotransmitters, maintain integrity and function of the blood–brain barrier and diminish inflammatory responses. Its suitability for safely treating RSE treatment in humans remains to be determined. Mild TTM has some benefits in SE but it rarely allows a sustained control of ongoing SE, since seizures tend to recur in normothermia,61 which justify exploring the use of lower temperatures. However, extensive evaluation of the efficacy and safety of mild and moderate TTM (32–34°C) will be needed before such deep TTM could be considered for human use.
- TTM for RSE is not given in the current guidelines.
- TTM is an option as third-tier treatment for SE.
- Remaining questions are:
– Is deep TTM using lower temperatures a possibility in humans?
– What are the effects of TTM on the metabolism of antiepileptic drugs?
– What are the side effects of mild, moderate or deep TTM, especially in patients with TBI?
Conclusions
The available evidence indicates that TTM has an important potential role in the treatment of various types of non-anoxic brain injury. This includes TBI, elevated ICP, SAH, ICH and refractory seizures. These are all conditions which usually have poor prognoses and new approaches to their management that would improve survival and reduce consequent disability are clearly needed. In vivo studies have provided valuable information on the mechanisms of brain injury and neuroprotection. They provide compelling data on the efficacy of cooling following an insult to the brain.
Further large-scale clinical trials focusing on TTM are required to better understand its role in non-anoxic brain injury. This is noted in the guidelines in which this lack of substantial clinical trial evidence prevents their stronger recommendation of TTM. The lack of data may, in part, be due to difficulties conducting controlled studies in critical care medicine in which urgent treatment needs can prevent normal patient recruitment procedures and adherence to study protocols. The existing guidelines suggest that TTM should be used after other interventions, with the result that only patients with the most difficult to-treat conditions are likely to receive it. Some studies indicate that TTM used earlier and even prophylactically can provide considerable benefits and some degree of neuroprotection.
The small-scale clinical trials and patient case reports indicate that TTM can be beneficial, although data supporting consistent efficacy and safety across different types of injury are still lacking. A few clinical trials are in progress to investigate TTM in brain injury such as the SNICH and TTM ICH studies, which are expected to report results soon. These may clarify the benefits of TTM approaches in larger patient populations. Until such investigations are conducted, TTM may remain an experimental procedure that is reserved for last resort interventions and its potential to reduce fever and ICP following brain injury and improve patient outcomes may not be fully realised.


