




Alzheimer’s disease (AD) is approaching epidemic proportions as the world’s population ages and the number of victims of this age-related disorder soars.1 At the same time that this tsunami of affected individuals looms, there has been little progress in developing new therapies, either symptomatic drugs to relieve the symptoms of AD or disease-modifying therapies (DMTs) to prevent, delay onset, or slow progression. No new novel treatment of AD has been approved since 2003 and 100% of DMTs in development have failed.2
Drug development progresses from preclinical studies in animals to phase I trials involving normal volunteers, to phase II “learning” trials in small populations of AD patients, to phase III confirmatory trials that demonstrate safety and efficacy prior to seeking marketing approval and making treatments widely available to patients. Phase II establishes proof-of-concept (POC) and determines the optimal doses to be included in phase III trials.3 Phase III is the longest phase of drug development, includes the largest number of patients, and consumes the largest share of resources. Thus, only agents that have demonstrated POC efficacy in phase II should be advanced to phase III. Stopping development of ineffective drugs in phase II will save resources that can be devoted to other projects and will save exposing patients to drugs and side effects in futile trials. Many drugs that have failed and many in the current AD pipeline have not shown POC in phase II before proceeding to phase III. A high failure rate can be anticipated among these agents.
A critical aspect of phase II POC is target engagement and proof of mechanism. Figure 1 shows how advances in understanding the biological underpinnings of human cognition can be applied to clinical trials to achieve POC in phase II. There is an ascending hierarchy of brain function from cells and cell processes, to circuit integration underlying cognitive function. In AD, amyloid-beta protein (Ab) and phosphorylated tau protein aggregate and form neuritic plaques and neurofibrillary tangles, respectively. Protein oligomerization and aggregation lead to cell death, inflammation, and apoptosis.4 Several biomarkers have been identified that provide insight into these events in the basic biology of AD. Brain imaging relevant to this level of understanding includes amyloid positron emission tomography (PET), tau PET, and atrophy as measured by magnetic resonance imaging (MRI). Fluid biomarkers reflective of these events include cerebrospinal fluid (CSF) Ab, CSF total tau protein, CSF phosphorylated tau (p-tau) protein, visinin-like protein 1 (VILIP1), and neurofilament light chain protein.5,6 CSF Ab production and clearance can be measured using stable isotope labeled kinetics (SILK) techniques.7
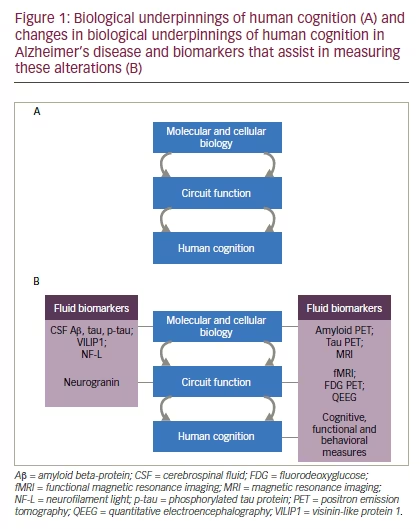
Human cognition depends on intact cortical circuitry and assessment of circuits may provide insight into drug effects at this critically important level of central nervous system (CNS) organization.8 Circuit function can be assessed with functional MRI (fMRI), fluorodeoxyglucose (FDG) PET, and quantitative electroencephalography (QEEG).9–11
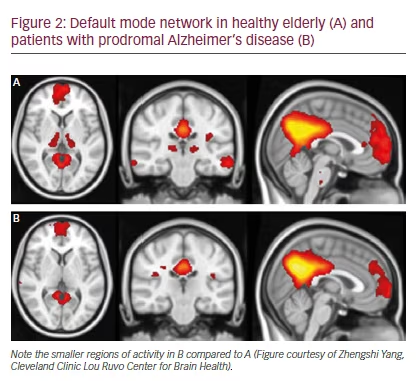
The technique that most clearly assesses circuit function is fMRI. Task-free resting state fMRI reveals a posterior default mode network (DMN) and an anterior salience network (SN). The DMN comprises a temporal-parietalhippocampal network associated with memory and visuospatial function; the SN includes frontal structures relevant to social-emotional function. In AD, the posterior DMN is preferentially affected, reflecting the temporalparietal patho-geography of the major histologic changes. DMN connectivity to posterior hippocampus and medial cingulo-parieto-occipital regions is diminished and SN connectivity is intensified.12 DMN changes are sensitive to the pathology of AD, present in prodromal AD,13 and anticipate cognitive abnormalities in individuals genetically predisposed to development of AD.14 Resting state measures show improved hippocampal connectivity in mild AD following treatment with donepezil that correlates with commonly used clinical trial measures.15 Figure 2 shows regions of DMN activity in normal elderly and in patients with prodromal AD (defined as mild cognitive impairment in amyloid-positive individuals).
These studies suggest that fMRI DMN provides insight into drug effects often currently lacking in phase II development programs. They may be relevant to both DMTs and symptomatic cognitive enhancing therapies. Abnormalities are detectable early, suggesting that they can be used in prevention trials of at-risk individuals and treatment trials of persons with prodromal AD or mild AD dementia. They are sensitive measures, allowing POC trials to be completed in shorter periods of time with smaller sample sizes than conventional phase II trials. Correlations with cognitive measures suggest that drugs or drug doses not improving DMN function in trials of cognitive enhancing agents or not preserving the function better than placebo in DMT trials are unlikely to produce a cognitive benefit in longer larger trials. Resting state measures are collected without asking participants to perform cognitive tasks and may be applicable to trials involving individuals across a broad range of severity and in global settings. Standard protocols will be required for multi-site trials, but relatively few specialized sites may be needed for POC studies.
An unresolved conundrum for phase II of drug development is whether to require demonstration of cognitive benefit.16 Trials designed to show robust clinical benefit must be large and long and therefore are similar or identical to trials required for phase III. Taking time to determine clinical responses consumes patent life, making long phase II trials untenable. This has led some sponsors to skip phase II, proceeding directly from animal studies and human safety trials to phase III. Within this paradigm, there is relatively little opportunity to understand the candidate treatment, explore dose relationships, accrue safety data, or collect biomarker data possibly predictive of phase III efficacy. Phase II trials measuring amyloid or tau burden or CSF measures involving Ab, tau, and p-tau may take longer to demonstrate and, even if positive but insufficient to affect circuit function, might not accurately forecast clinical benefit. DMN measure relates directly to cognitive function and may optimize demonstration of POC in phase II.
The fMRI technique has not been established as a surrogate measure that predicts clinical outcomes. We suggest that the current data warrant further investigation and that development programs explore the potential utility of DMN measures to assess drug and dose effects systematically and to determine if this approach, when incorporated in phase II, allows better prediction of phase III outcomes.


