Neurocognitive function is commonly compromised in cancer patients. While symptoms can be caused by the tumor itself and are commonly seen in patients with brain tumors, the etiology of neurocognitive deficits is much more complex in patients treated for tumors outside the nervous system.
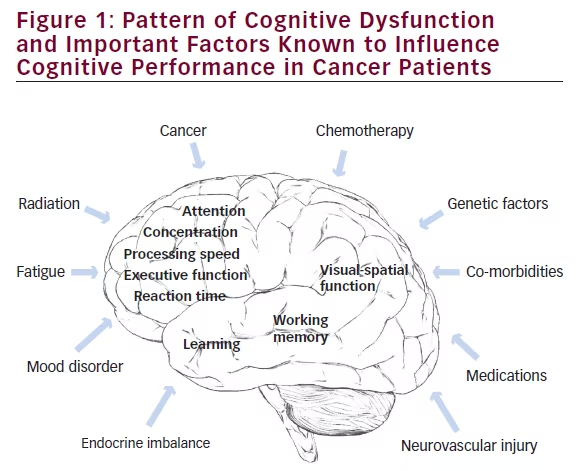
Impaired cognition can be present in cancer patients prior to treatment; however, treatment related adverse effects from c hemotherapy and radiation are well known to cause harmful effects on the brain and play a significant role in the development and progression of neurocognitive symptoms.1 In addition, various co-morbidities, mood and sleeping disorders, and medication effects can affect neurocognitive function (see Figure 1). It therefore can be difficult to delineate the exact contribution of each of these factors in clinical practice, posing a significant challenge to patient management.
As disruption in neurocognitive function can be a major cause of impaired quality of life, attention to these symptoms and consideration of possible therapeutic interventions directed to improve neurocognitive deficits have become increasingly important in clinical oncology and cancer survivorship.
Chemotherapy Effects on Neurocognitive
Function The most frequently described neurocognitive problems in patients treated with various chemotherapy regimens include memory and learning deficits, alterations of attention, concentration, processing speed and executive function.2
Symptoms can be of delayed onset and progressive for years after cessation of tumor therapy. While neurocognitive adverse effects from chemotherapy have long been recognized in long-term survivors of childhood cancer,3,4 adult cancer patients can be equally affected, and chemotherapy associated cognitive dysfunction appears to be more common than previously anticipated.1,5-8 Cognitive dysfunction has been reported in 15–95% of patients treated with chemotherapy,5,6,9 depending on study design, patient population and the battery of neuropsychological tests administered. While cognitive impairment has been confirmed in patients treated for various cancer types,10–12 most compelling studies were done in breast cancer patients, of whom 20–40% show cognitive deficits on post-treatment evaluation.6,8,13–18 Symptoms might be of delayed onset and follow a progressive pattern. Approximately 30–60% of breast cancer survivors demonstrate cognitive deficits even up to 20 years after active cancer therapy.18–20
Experimental studies have revealed insights into the underlying mechanisms of cognitive dysfunction in cancer patients. Specifically, a large number of animal studies have discovered the cell-biological effects of various chemotherapeutic drugs on the central nervous system.21 Neurocognitive adverse effects have been observed with all categories of chemotherapeutic
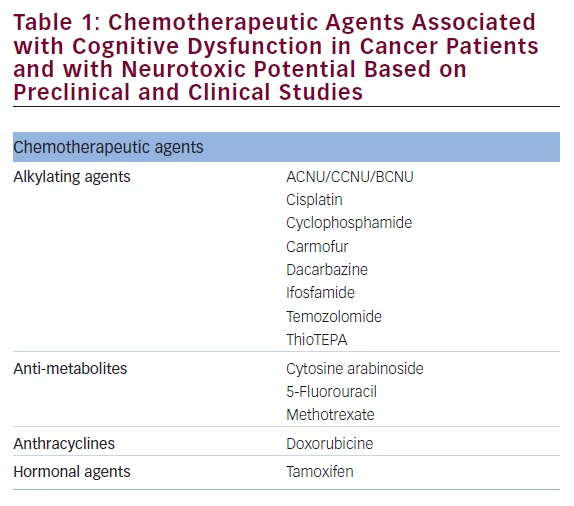
agents tested (see Table 1).22 Potential mechanisms include chemotherapy associated direct cellular toxicity, alterations in cellular metabolism, oxidative stress, and induction of pro-inflammatory processes with subsequent disruption of normal cellular and neurological function.23–29
The current body of literature suggests that disruption of neural progenitor cells required for maintenance of brain plasticity throughout life and impairment of hippocampal neurogenesis are important etiologic factors underlying behavioral and cognitive abnormalities.21,30–35 However, effects of chemotherapy on the nervous system have mostly been studied in non-tumor bearing rodent models, and have therefore not been able to address the concern that the tumor itself might influence neurocognitive function, as suggested by some clinical studies.
Nevertheless, chemotherapy-induced damage to neural progenitor cells has offered a compelling explanation for delayed and progressive neurotoxic effects of chemotherapy.
Clinical studies have shown that the risk of developing neurocognitive symptoms is also influenced by metabolic alterations, hormonal changes, the level of cognitive function prior to treatment and other medical co-morbidities, and genetic factors.1,36–42
Figure 1 summarizes the most common neurocognitive deficits reported in cancer patients and illustrates various conditions and clinically relevant factors known to influence cognitive performance and that need to be considered in clinical management.
In light of the spectrum of neurocognitive symptoms encountered in cancer patients and the increasingly recognized cell-biological effects of chemotherapy on the brain, some authors have proposed the concept of accelerated aging of the nervous system as a consequence of chemotherapy.43
Diagnostic and Therapeutic Considerations
Assessment of neurocognitive function requires reliable, quantifiable, and valid measures, sensitive to cognitive and quality of life deficits in cancer patients. Testing strategies that closely relate to real-life situations, in which cognitive deficits readily manifest, are considered most relevant. Several guidelines have been developed regarding the selection of neuropsychological tests that efficiently capture cognitive function and that can be uniformly applied to cancer patients.8,44–46 In addition, the identification of novel biomarkers to identify and monitor chemotherapy associated cognitive changes remains an important objective of ongoing investigations. Recent translational imaging studies using structural and functional magnetic resonance imaging (MRI) have identified compelling evidence for chemotherapy-related brain changes.47
There are currently no standard therapies for patients who experience cognitive symptoms following chemotherapy. Therapeutic interventions may include strategies to either prevent side effects, or to minimize the severity of symptoms. For instance, neurostimulants, such as methylphenidate48–50 and modafenil51,52 are promising agents for treatment of cancer therapy related cognitive dysfunction. In addition, donepezil – a reversible acetylcholinesterase inhibitor used to treat Alzheimer’s type dementia – has shown to improve cognitive function, mood, and quality of life in patients with brain and small cell lung cancer.53,54
Optimal management of fatigue, mood disorders and other co-morbidities need to be integral part of patient management. Notably, treatment of a sleep disorder or depression may eliminate cognitive deficits if those disorders are the primary cause. Cognitive and behavioral intervention strategies may also be employed in patients with chemotherapy associated cognitive dysfunction.55 These interventions often focus on compensatory strategies, stress management, energy conservation and psycho-education. External memory aids (e.g., memory notebooks, pagers) have been among the most widely used interventions.56
Other non-pharmacological interventions include meditation,57 exercise,58,59 and regulation of sleep.60
Challenges and Outlook
Numerous preclinical and translational neuroimaging studies in cancer patients have started to shed light on the structural and functional impact of chemotherapy on the brain.61
However, translating these findings into clinical practice has remained challenging.
Improved study design (e.g., longitudinal and prospective, use of comparable testing batteries and incorporation of advanced neuroimaging protocols), and study of more homogenous patient populations with comparable treatment regimens in clinical trials will be important to obtain more conclusive evidence on the impact of chemotherapy on the brain. Importantly, not all patients experience neurotoxic adverse effects of chemotherapy, and significant heterogeneity exists in the degree of symptoms among affected cancer patients.
To delineate the exact mechanisms of how chemotherapy alters brain function and to identify associated risk factors will help to develop brain repair strategies that can be incorporated into clinical practice.
References
1. Dietrich J, Monje M, Wefel J, et al., Clinical patterns and biological correlates of cognitive dysfunction associated with cancer therapy, Oncologist, 2008;13(12):1285–95.
2. Lindner OC, Phillips B, McCabe MG, et al., A meta-analysis of cognitive impairment following adult cancer chemotherapy, Neuropsychology, 2014;28(5):726–40.
3. Butler RW, Haser JK, Neurocognitive effects of treatment for childhood cancer. Ment Retard Dev Disabil Res Rev, 2006;12(3):184–91.
4. Alvarez JA, Scully RE, Miller TL, et al., Long-term effects of treatments for childhood cancers. Curr Opin Pediatr, 2007;19(1):23–31.
5. Ahles TA, Saykin A, Cognitive effects of standard-dose chemotherapy in patients with cancer, Cancer Invest, 2001;19(9):812–20.
6. Wefel JS, Lenzi R, Theriault RL, et al., The cognitive sequelae of standard-dose adjuvant chemotherapy in women with breast carcinoma: results of a prospective, randomized, longitudinal trial, Cancer, 2004;100(11):2292–9.
7. Schagen SB, Muller MJ, Boogerd W, et al., Change in cognitive function after chemotherapy: a prospective longitudinal study in breast cancer patients, J Natl Cancer Inst, 2006;98(23):1742–5.
8. Vardy J, Wefel JS, Ahles T, et al., Cancer and cancer-therapy related cognitive dysfunction: an international perspective from the Venice cognitive workshop, Ann Oncol, 2008;19(4):623–9.
9. Moleski M, Neuropsychological, neuroanatomical, and neurophysiological consequences of CNS chemotherapy for acute lymphoblastic leukemia, Arch Clin Neuropsychol, 2000;15(7):603–30.
10. Jansen CE, Miaskowski C, Dodd M, et al., A metaanalysis of studies of the effects of cancer chemotherapy on various domains of cognitive function, Cancer, 2005;104(10):2222–33.
11. Hess LM, Chambers SK, Hatch K, et al., Pilot study of the prospective identification of changes in cognitive function during chemotherapy treatment for advanced ovarian cancer, J Support Oncol, 2010;8(6):252–8.
12. Wefel JS, Vidrine DJ, Marani SK, et al., A prospective study of cognitive function in men with non-seminomatous germ cell tumors, Psychooncology, 2014;23(6):626–33.
13. Heflin LH, Meyerowitz BE, Hall P, et al., Cancer as a risk factor for long-term cognitive deficits and dementia, J Natl Cancer Inst, 2005;97(11):854–6.
14. Wefel JS, Meyers CA, Cancer as a risk factor for dementia: a house built on shifting sand, J Natl Cancer Inst, 2005;97(11):788–9.
15. Hermelink K, Untch M, Lux MP, et al., Cognitive function during neoadjuvant chemotherapy for breast cancer: results of a prospective, multicenter, longitudinal study, Cancer, 2007;109(9):1905–13.
16. Vardy J, Rourke S, Tannock IF, Evaluation of cognitive function associated with chemotherapy: a review of published studies and recommendations for future research, J Clin Oncol, 2007;25(17):2455–63.
17. Jansen CE, Dodd MJ, Miaskowski CA, et al., Preliminary results of a longitudinal study of changes in cognitive function in breast cancer patients undergoing chemotherapy with doxorubicin and cyclophosphamide, Psychooncology, 20058;17(12):1189–95.
18. Wefel JS, Saleeba AK, Buzdar AU, et al: Acute and late onset cognitive dysfunction associated with chemotherapy in women with breast cancer. Cancer 116:3348–56, 2010
19. Hutchinson AD, Hosking JR, Kichenadasse G, et al., Objective and subjective cognitive impairment following chemotherapy for cancer: a systematic review, Cancer Treat Rev, 2012;38(7):926–34.
20. Koppelmans V, Breteler MM, Boogerd W, et al., Neuropsychological performance in survivors of breast cancer more than 20 years after adjuvant chemotherapy, J Clin Oncol, 2012;30(10):1080–6.
21. Seigers R, Schagen SB, Van Tellingen O, et al., Chemotherapyrelated cognitive dysfunction: current animal studies and future directions, Brain Imaging Behav, 2013;7(4):453–9
22. Dietrich J, Wen P, Neurologic complications of chemotherapy. In: Schiff D, Kesari S, Wen P (eds), Cancer Neurology in Clinical Practice (ed 2nd.), Totowa, New Jersey: Humana Press Inc., 2008;287–326
23. Hook CC, Kimmel DW, Kvols LK, et al., Multifocal inflammatory leukoencephalopathy with 5-fluorouracil and levamisole, Ann Neurol, 1992;31(3):262–7.
24. Lai R, Abrey LE, Rosenblum MK, et al., Treatment-induced leukoencephalopathy in primary CNS lymphoma: a clinical and autopsy study, Neurology, 2004;62(3):451–6.
25. Kaya E, Keskin L, Aydogdu I, et al: Oxidant/antioxidant parameters and their relationship with chemotherapy in Hodgkin’s lymphoma, J Int Med Res, 2005;33(6):687–92.
26. Papageorgiou M, Stiakaki E, Dimitriou H, et al., Cancer chemotherapy reduces plasma total antioxidant capacity in children with malignancies, Leuk Res, 2005;29(1):11–6.
27. Kennedy DD, Ladas EJ, Rheingold SR, et al., Antioxidant status decreases in children with acute lymphoblastic leukemia during the first six months of chemotherapy treatment, Pediatr Blood Cancer, 2005;44(4):378–85
28. Perry A, Schmidt RE, Cancer therapy-associated CNS neuropathology: an update and review of the literature, Acta Neuropathol, 2006;111(3):197–212.
29. Noble M, Mayer-Proschel M, Li Z, et al., Redox biology in normal cells and cancer: restoring function of the redox/Fyn/c-Cbl pathway in cancer cells offers new approaches to cancer treatment, Free Radic Biol Med, 2015;79:300–23.
30. Dietrich J, Han R, Yang Y, et al., CNS progenitor cells and oligodendrocytes are targets of chemotherapeutic agents in vitro and in vivo, J Biol, 2006;5(7):22.
31. Han R, Yang YM, Dietrich J, et al., Systemic 5-fluorouracil treatment causes a syndrome of delayed myelin destruction in the central nervous system, J Biol, 2008;7(4):12.
32. Seigers R, Schagen SB, Beerling W, et al., Long-lasting suppression of hippocampal cell proliferation and impaired cognitive performance by methotrexate in the rat, Behav Brain Res, 2008;186(2):168–75.
33. Fardell JE, Vardy J, Logge W, et al., Single high dose treatment with methotrexate causes long-lasting cognitive dysfunction in laboratory rodents, Pharmacol Biochem Behav, 2010;97(2):333–9
34. Monje M, Dietrich J, Cognitive side effects of cancer therapy demonstrate a functional role for adult neurogenesis, Behav Brain Res, 2012;227(2):376–9.
35. Dietrich J, Prust M, Kaiser J, Chemotherapy, cognitive impairment and hippocampal toxicity, Neuroscience, 2015;309:224–32.
36. Ahles TA, Saykin AJ, Noll WW, et al., The relationship of APOE genotype to neuropsychological performance in long-term cancer survivors treated with standard dose chemotherapy, Psychooncology, 2003;12(6):612–9.
37. McAllister TW, Ahles TA, Saykin AJ, et al., Cognitive effects of cytotoxic cancer chemotherapy: pre-disposing risk factors and potential treatments, Curr Psychiatry Rep, 2004;6(5):364–71.
38. Muramatsu T, Johnson DR, Finch RA, et al., Age-related differences in vincristine toxicity and bio-distribution in wildtype and transporter-deficient mice, Oncol Res, 2004;14(7– 8):331–43.
39. Linnebank M, Pels H, Kleczar N, et al., MTX-induced white matter changes are associated with pol-ymorphisms of methionine metabolism, Neurology, 2005;64(5):912–3.
40. Krajinovic M, Robaey P, Chiasson S, et al., Polymorphisms of genes controlling homocysteine levels and IQ score following the treatment for childhood ALL, Pharmacogenomics, 2005;6(3):293–302.
41. Fishel ML, Vasko MR, Kelley MR, DNA repair in neurons: so if they don’t divide what’s to repair?, Mutat Res, 2007;614(1–2):24–36.
42. Ahles TA, Saykin AJ, Candidate mechanisms for chemotherapyinduced cognitive changes, Nat Rev Cancer, 2007;7(3):192–201.
43. Ahles TA, Root JC, Ryan EL, Cancer- and cancer treatment associated cognitive change: an update on the state of the science, J Clin Oncol, 2012;30(30):3675–86.
44. Abrey LE, Batchelor TT, Ferreri AJ, et al., Report of an international workshop to standardize baseline evaluation and response criteria for primary CNS lymphoma, J Clin Oncol, 2005;23(22):5034–43.
45. Correa DD, Maron L, Harder H, et al., Cognitive functions in primary central nervous system lymphoma: literature review and assessment guidelines, Ann Oncol, 2007;18(7):1145–51.
46. Krull KR, Okcu MF, Potter B, et al., Screening for neurocognitive impairment in pediatric cancer long-term survivors, J Clin Oncol, 2008;26(25):4138–43.
47. Kaiser J, Bledowski C, Dietrich J, Neural correlates of chemotherapy-related cognitive impairment, Cortex, 2014;54:33–50.
48. Conklin HM, Khan RB, Reddick WE, et al., Acute neurocognitive response to methylphenidate among survivors of childhood cancer: a randomized, double-blind, cross-over trial, J Pediatr Psychol, 2007;32(9):1127–39.
49. Mulhern RK, Khan RB, Kaplan S, et al., Short-term efficacy of methylphenidate: a randomized, double-blind, placebocontrolled trial among survivors of childhood cancer, J Clin Oncol, 2004;22(23):4795–803.
50. Meyers CA, Weitzner MA, Valentine AD, et al., Methylphenidate therapy improves cognition, mood, and function of brain tumor patients, J Clin Oncol, 1998;16(7):2522–7.
51. Kohli S, Fisher SG, Tra Y, et al., The effect of modafinil on cognitive function in breast cancer survivors, Cancer, 2009;115(12):2605–16.
52. Lundorff LE, Jonsson BH, Sjogren P, Modafinil for attentional and psychomotor dysfunction in advanced cancer: a double-blind, randomised, cross-over trial, Palliat Med, 2009;23(8):731–8.
53. Jatoi A, Kahanic SP, Frytak S, et al., Donepezil and vitamin E for preventing cognitive dysfunction in small cell lung cancer patients: preliminary results and suggestions for future study designs, Support Care Cancer, 2005;13(1):66–9.
54. Rapp SR, Case LD, Peiffer A, et al., Donepezil for Irradiated Brain Tumor Survivors: A Phase III Randomized Placebo-Controlled Clinical Trial, J Clin Oncol, 2015;33(15):1653–9.
55. Ferguson RJ, Ahles TA, Saykin AJ, et al., Cognitive-behavioral management of chemotherapy-related cognitive change, Psychooncology, 2007;16(8):772–7.
56. Evans JJ, Wilson BA, Needham P, et al., Who makes good use of memory aids? Results of a survey of people with acquired brain injury, J Int Neuropsychol Soc, 2003;9(6):925–35.
57. Biegler KA, Chaoul MA, Cohen L, Cancer, cognitive impairment, and meditation, Acta Oncol, 2009;48(1):18–26.
58. Hsieh CC, Sprod LK, Hydock DS, et al., Effects of a supervised exercise intervention on recovery from treatment regimens in breast cancer survivors, Oncol Nurs Forum, 2008;35(6):909–15.
59. Mitchell SA, Cancer-related fatigue: state of the science. PM R 2010;2:364–83.
60. Berger AM, Update on the state of the science: sleep-wake disturbances in adult patients with cancer, Oncol Nurs Forum, 2009;36(4):E165–77.
61. Saykin AJ, de Ruiter MB, McDonald BC, et al., Neuroimaging biomarkers and cognitive function in non-CNS cancer and its treatment: current status and recommendations for future research, Brain Imaging Behav, 2013;7(4):363–73.







